Скачать с ютуб Knee Pain, Meniscal Tear Diagnosis & MRI - Everything You Need To Know - Dr. Nabil Ebraheim в хорошем качестве
Knee Pain, Meniscal Tear Diagnosis & MRI - Everything You Need To Know - Dr. Nabil Ebraheim
7 лет назад
Скачать бесплатно и смотреть ютуб-видео без блокировок Knee Pain, Meniscal Tear Diagnosis & MRI - Everything You Need To Know - Dr. Nabil Ebraheim в качестве 4к (2к / 1080p)
У нас вы можете посмотреть бесплатно Knee Pain, Meniscal Tear Diagnosis & MRI - Everything You Need To Know - Dr. Nabil Ebraheim или скачать в максимальном доступном качестве, которое было загружено на ютуб. Для скачивания выберите вариант из формы ниже:
Загрузить музыку / рингтон Knee Pain, Meniscal Tear Diagnosis & MRI - Everything You Need To Know - Dr. Nabil Ebraheim в формате MP3:
Если кнопки скачивания не
загрузились
НАЖМИТЕ ЗДЕСЬ или обновите страницу
Если возникают проблемы со скачиванием, пожалуйста напишите в поддержку по адресу внизу
страницы.
Спасибо за использование сервиса savevideohd.ru
Knee Pain, Meniscal Tear Diagnosis & MRI - Everything You Need To Know - Dr. Nabil Ebraheim
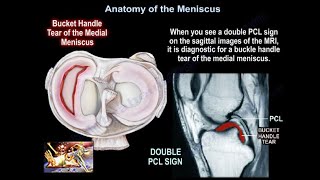
Dr. Ebraheim’s educational animated video describes knee pain and its indications. The patient will come to you with a history of a twisting injury and pain around the knee. The patient may give you a history of mechanical symptoms, such as: locking, clicking, or some swelling. You examine the patient and you’ll find there is joint line tenderness, maybe some effusion, and mcmurray’s test may be positive; Painful click is obtained at the knee is brought by flexion to extension with internal or external rotation. This maneuver also helps you to differentiate if the meniscus tear is on the medial or lateral side. Treatment: • NSAIDS • Physical Therapy • Injections • If there is no improvement, get an MRI. • You get the MRI early if patient has locked knee, means: you don’t have full extension of the knee, or if there is blood in the knee, so when you aspirate the knee because there is an effusion you get blood and you suspect ACL, you get an MRI. • In this situation you will suspect lateral meniscal tear. • It is usually a vertical tear of the posterior horn of the lateral meniscus and it is the commonly missed tear on an MRI. • Get x-ray first before you get an MRI to check if there is a fracture, arthritis, or any other problems in the knee. Why do you get an MRI? Because the clinical diagnosis accuracy is about 70%, and because there are other issues on the knee that can give you the same symptoms like the meniscal tear. These things may be intra articular or extra articular, and the symptoms will mimic meniscal tear, so we get the MRI, and it is the most sensitive test. You need to know these facts: • The lateral meniscus has twice the excursion of the medial meniscus, that’s why the medial meniscal tear is three times more often to occur than the lateral meniscus, so look for a tear of the medial meniscus because it is more common than the lateral meniscus. • Also the lateral meniscus will have most of the meniscal cyst. • On an MRI, how do you know which is the lateral meniscus? Check the position of the fibula, the lateral meniscus is on the same side as the fibula, also note that the fibula is posterior. • MRI is the best study to diagnose or to confirm meniscal pathology. • What do you see on the MRI? A normal meniscus will be dark; in the video we can see how we make these cuts in the MRI of the meniscus. The globular intrasubstance signal: • This increased signal intensity is within the meniscus, but it doesn’t extend to the surface of the meniscus in the grade I tear. • In grade II tear: you will have a linear area increased signal intensity, its inside the meniscus, and it does not go to the surface of the meniscus. • In grade III tear: you can see that the tear extends to the articular surface. What are the MRI signs of the meniscal tear? • Grade III signal, extend to the surface of the meniscus, among other things., example: may be horizontal, vertical, radial, oblique, complex, could be degenerative, displaced or missing a fragment, it can be in different forms and types, but there are a few important things in the MRI worth mentioning, this material frequently comes in the examinations, and they are: 1- The double PCL sign, the bucket handle tear of the medial meniscus, it is seen on the sagittal MRI, when a torn meniscal fragment is flipped and displaced into the notch, it’s a 100% specific for a flip bucket handle medial meniscal tear. 2- On the other hand bucket handle tear of the lateral meniscus where the posterior horn of the lateral meniscus flips anteriorly you will see the double anterior horn sign. What are the false positives in the MRI? 1- There’s a ligament called the transverse meniscal ligament, which attaches to the anterior horn of the lateral meniscus, and this one mimics the meniscal tear. 2- There is also a meniscofemoral ligament, attaches to the superior horn of the lateral meniscus, and this one also mimics meniscal tear. It is the humphrey or the wrisberg ligament. 3- Also if you have fluid tracking onto the sheath of the popliteal tendon, it will mimic posterior horn lateral meniscal tear. 4- Discoid meniscus: it is common in the lateral meniscus, patient will have a history of clicking or locking, or history of lack of full knee extension, patient will have more than 2 bowties, and the meniscus will extend beyond the half-way point of the condyle. 5- Parameniscal cysts: if you see it, you could have meniscal tear, especially with lateral meniscus horizontal tear, for this condition you will do partial meniscectomy and decompression of the cyst, the differential diagnosis will be: ganglion cyst and bursitis. 6- Baker’s cyst: you could have a combination of meniscal tear and baker’s cyst, it does not mean you have a meniscal tear,
Comments