Скачать с ютуб Anatomy Of The Rotator Cuff Muscles - Everything You Need To Know - Dr. Nabil Ebraheim в хорошем качестве
Anatomy Of The Rotator Cuff Muscles - Everything You Need To Know - Dr. Nabil Ebraheim
7 лет назад
rotator cuff muscles
supraspinatus
infraspinatus
subscapularis
rotator cuff assessment
the rotator cuff MRI
ROTATOR CUFF INJURY
rotator cuff anatomy
rotator cuff tear
rotator cuff surgery
rotator cuff stretches
rotator cuff rehab
rotator cuff muscle function
rotator cuff muscle anatomy
rotator cuff muscle pain
rotator cuff muscle exercises
rotator cufff muscle tear
rotator cuff muscle pain relief
rotator cuff muscle surgery
rotator cuff muscle testing
Скачать бесплатно и смотреть ютуб-видео без блокировок Anatomy Of The Rotator Cuff Muscles - Everything You Need To Know - Dr. Nabil Ebraheim в качестве 4к (2к / 1080p)
У нас вы можете посмотреть бесплатно Anatomy Of The Rotator Cuff Muscles - Everything You Need To Know - Dr. Nabil Ebraheim или скачать в максимальном доступном качестве, которое было загружено на ютуб. Для скачивания выберите вариант из формы ниже:
Загрузить музыку / рингтон Anatomy Of The Rotator Cuff Muscles - Everything You Need To Know - Dr. Nabil Ebraheim в формате MP3:
Если кнопки скачивания не
загрузились
НАЖМИТЕ ЗДЕСЬ или обновите страницу
Если возникают проблемы со скачиванием, пожалуйста напишите в поддержку по адресу внизу
страницы.
Спасибо за использование сервиса savevideohd.ru
Anatomy Of The Rotator Cuff Muscles - Everything You Need To Know - Dr. Nabil Ebraheim
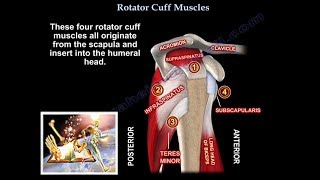
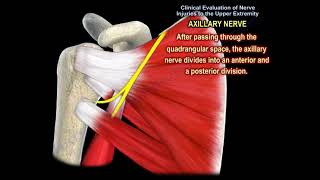
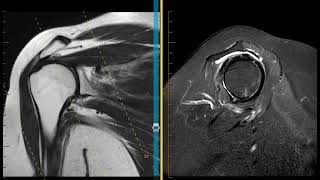
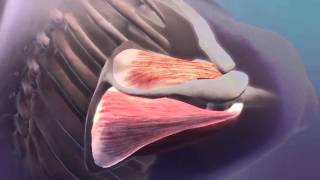
Dr. Ebraheim’s educational animated video illustrates the shoulder rotator cuff muscles and associated tears .Dr. Ebraheim animated video illustrates the shoulder rotator cuff muscles and types of imaging for these injuries.it is a shoulder animation video that explains the rotator cuff anatomy , the rotator cuff MRI , ROTATOR CUFF INJURY ,TEAR IS explained .rotator cuff surgery is also explained .rotator cuff rehab is important .The video explains the anatomy of the rotator cuff in relation to rotator cuff nerve supply ,rotator cuff function and rotator cuff action. Rotator cuff is a group of four muscles that lifts and rotates the arm at the shoulder area. The rotator cuff muscles originate at the scapula and insert into the head of the humerus. Rotator cuff tears are a common source of shoulder pain. When the rotator cuff is torn, the patient will complain of a painful, weak shoulder. The patient will not be able to lift or rotate the arm with the same range of motion or strength as before the injury. The patient will have a significant pain associated with motion of the shoulder and the pain is common at night, radiating to the arm. Rotator cuff tear is usually diagnosed by clinical examination and confirmed by getting an MRI. Treatment: NSAIDS. Physical therapy. Injection. Surgery: • Surgery is done when the tear is traumatic and when there is failure of conservative treatment. Complete tear of the rotator cuff will not heal without surgery. The tendon will need to be repaired by suturing the tendon back to the humerus. Utilize sutures or bone anchors. The operation can be done arthroscopically, open, or also done by a combination of both with a small incision. Some tears are greater than 5cm in size and involve multiple tendons. These massive tears usually occur in elderly patients. Sometimes the rotator cuff muscles will have atrophy and fatty infiltration. These are the patients who will have a poor outcome. With smaller tears, surgical repair is more successful. In traumatic tears, the sooner the repair the better the outcome. The rotator cuff is a dynamic stabilizer by tensioning, contracting, and holding the humeral head tightly within the glenoid cavity as the shoulder moves. There are four muscles of the rotator cuff: 1- Subscapularis. 2- Supraspinatus. 3- Infraspinatus. 4- Teres minor. The supraspinatus and the infraspinatus receive innervation from the suprascapular nerve which is the only nerve that arises from the upper trunk. The subscapularis will get innervation from the upper and lower subscapular nerve from the posterior cord of the brachial plexus. The teres minor will get innervation from the axillary nerve which comes from the posterior cord of the brachial plexus. • Supraspinatus: Origin is located on the superior aspect of the scapula above the scapular spine and inserts into the greater tubercle of the humerus. Function: If you want to know the function of all the rotator cuff muscles, then take a look at their insertion. So according to its insertion, the function of the supraspinatus muscle is to initiate the abduction of the arm, so when you test this muscle you will find that when it is torn, you will have weak abduction and drop arm test. • Infraspinatus: Origin: below the spine of the scapula and inserts posteriorly into the greater tuberosity of the humerus. This muscle is the primary external rotator of the humerus. If this muscle is torn, the patient will have weak external rotation with the arm to the side. • Teres Minor: Origin: from the middle half of the lateral border of the scapula and it inderts into the humeral head inferior to the infraspinatus muscle. Function: external rotation of the humerus. It is tested by weak Horn Blowers Sign, which is weakness of external rotation at 90° of abduction. • Subscapularis: If the subscapularis rupture, it goes medially and the biceps tendon will be dislocated or subluxed and goes medially also. Originates from the subscapularis fossa and inserts on the lesser tuberosity of the humerus. Function: internal rotation of the humerus. When this muscle ruptures it usually happen acutely similar to an avulsion in young oatients with hyperabduction and external rotation. It can also happen post operatively from failure of the repair after surgical procedure on the anterior shoulder area. Sometimes it is a tough diagnosis that could be missed, and if the condition becomes a chronic tear, you will probably need to do pectoralis major muscle transfer. Subscapularis tear is diagnosed via these two tests: Lift- Off Test: it test the upper subscapularis muscle (impotant part). The patient will be unable to hold the hand behind the back. Belly Press Test: it tests the lower subscapularis. The third test with the subscapularis test is excessive passive external rotation of the shoulder compared to the other shoulder.
Comments