Скачать с ютуб Abdominal Dermatomes and Referred Pain в хорошем качестве
Abdominal Dermatomes and Referred Pain
7 лет назад
Скачать бесплатно и смотреть ютуб-видео без блокировок Abdominal Dermatomes and Referred Pain в качестве 4к (2к / 1080p)
У нас вы можете посмотреть бесплатно Abdominal Dermatomes and Referred Pain или скачать в максимальном доступном качестве, которое было загружено на ютуб. Для скачивания выберите вариант из формы ниже:
Загрузить музыку / рингтон Abdominal Dermatomes and Referred Pain в формате MP3:
Если кнопки скачивания не
загрузились
НАЖМИТЕ ЗДЕСЬ или обновите страницу
Если возникают проблемы со скачиванием, пожалуйста напишите в поддержку по адресу внизу
страницы.
Спасибо за использование сервиса savevideohd.ru
Abdominal Dermatomes and Referred Pain
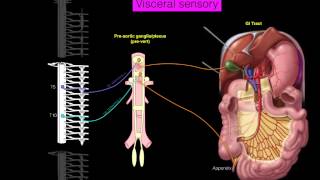
This is the third in a series of four videos that goes over how to memorize the dermatomes, or the area of skin supplied by nerves from a single spinal root. This video focuses on two concepts, first: the thoracic dermatomes, and second: the body’s localization of referred pain. In the first video in the series, I covered the cervical dermatomes as well as the first two thoracic. To recap, T1 provides sensory information from the medial forearm, and T2 provides sensory information from the armpit, also known as the axilla. The rest of the thoracic dermatomes are very easy. T3 through T12 are arranged in order down the trunk. The two landmarks you should know are first: the nipples at T4, and the umbilicus at T10. Now for referred pain. For many people, they first encounter this concept when they hear (or experience) the symptoms of a heart attack. The heart is located inside the thorax, but the heart attack is felt in the neck, shoulder, and back, and can even radiate to the jaw or the left arm. Interestingly, the biological mechanism of referred pain is not fully understood. http://journals.lww.com/clinicalpain/... One thought, called the convergent-projection theory, is that the first order nociceptive fibers from the local site (such as the heart) projects onto the same second order neurons in the spinal cord as the neurons from the referred site. However, this does not explain two key features of referred pain, that is, how referred pain has a delayed appearance from the onset of the insult, and how referred pain is unidirectional. One cannot produce pain in the shoulder and have it radiate up to the jaw, for example. Referred pain from a heart attack only occurs one way. Maybe another idea, known as both convergence-facilitation and central sensitization, could explain these phenomena. This theory supposes that the local pain projects to both two secondary pathways in the spinal cord, the second being shared with the referred pain site. The second projection might also have a different threshold to explain the delayed appearance. The different threshold idea is also called central hyperexcitability, which importantly explains the extent of the referred pain as well. Experiments have shown that size of referred pain area is directly related to the intensity and duration of evoked injury at the local site. Yet another idea supposes the convergence is higher up, known as the thalamic-convergence theory. This theory is supported by evidence of convergence of several pathways upon separate cortical and subcortical neurons in pain studies performed on monkeys. Aside from the example of the heart we just discussed, there are three other important areas of referred pain that are important to know as a medical student. The diaphragm is innervated by the phrenic nerve, and the phrenic nerve is supplied by nerve roots C3, 4, and 5. When an adjacent organ is injured or becomes inflamed, the diaphragm is also affected and refers pain to the shoulder. Liver and gallbladder pathology refers to the right shoulder, and spleen pathology refers to the left shoulder. Pancreas pathology refers to the front and the back overlying its location. Kidney pathology does the same, specifically to the costo-vertebral angle on the back, then extends with ureter pathology to the groin. Thanks for watching! Be sure to like and subscribe for more videos.
Comments